Presented by:
Steven E. Kahn, MD
University of Washington, Seattle, WA, USA Nikolaus Marx, MD
University Hospital Aachen, Aachen, Germany Darren K. McGuire, MD
University of Texas Southwestern Medical Center, Dallas, TX, USA Christoph Wanner, MD
Würzburg University Clinic, Würzburg, Germany Mark E. Cooper, MD
Monash University, Melbourne, Australia
CARMELINA was specifically designed to evaluate the cardiovascular (CV) (3P-MACE; CV death, non-fatal MI, non-fatal stroke) and kidney safety profile of linagliptin.
CARMELINA is the first CV outcomes trial to specifically assess the kidney safety profile of a dipeptidyl peptidase 4 (DPP-4) inhibitor.
Previous CV outcome trials of DPP-4 inhibitors have demonstrated a noninferior risk of a composite CV outcome vs. placebo, but not incremental CV efficacy. These prior trials evaluating DPP-4 inhibitors enrolled limited numbers of patients with concomitant chronic kidney disease, who are at very high CV risk. CARMELINA (CArdiovascular and Renal Microvascular outcomE study with LINAgliptin) is the first CV outcomes trial that specifically assessed the renal safety profile of a DPP-4 inhibitor, namely linagliptin.
The CARMELINA trial was designed to evaluate the CV safety and kidney outcomes of linagliptin in patients with type 2 diabetes at high cardiorenal risk.
Randomized, double-blind, placebo-controlled, multicenter noninferiority trial conducted at 605 clinic sites in 27 countries.
The trial enrolled adults with type 2 diabetes, HbA1c 6.5-10.0%.
Participants also had high CV risk (history of vascular disease and urine-albumin creatinine ratio (UACR( >200mg/g) and high renal risk (reduced eGFR and micro- or macroalbuminuria; end-stage kidney disease (ESKD) was excluded).
Patients were randomized to receive linagliptin (5 mg once daily; n=3,494) or placebo (n=3,485) added to usual care.
Other glucose-lowering medications or insulin could be added based on clinical need and local clinical guidelines.
Primary outcome measure
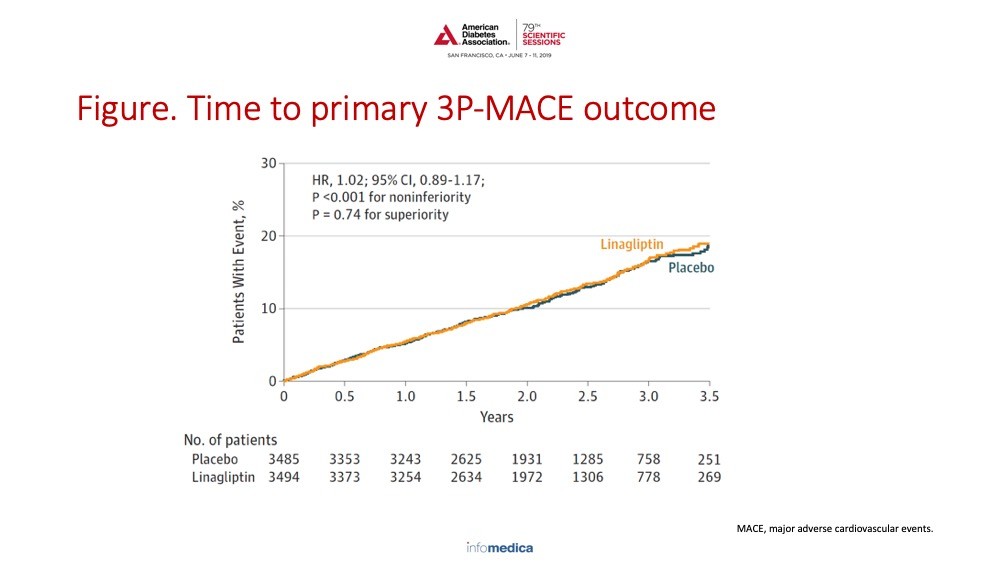
Primary outcome was time to first occurrence of the composite of CV death, nonfatal MI, or nonfatal stroke (3P-MACE) (Figure).
Criteria for noninferiority of linagliptin vs. placebo was defined by the upper limit of the 2-sided 95% CI for the HR of linagliptin relative to placebo being less than 1.3.
The primary outcome occurred in 12.4% and 12.1% of patients in the linagliptin and placebo groups, respectively (absolute incidence rate difference, 0.13 (95% CI −0.63 to 0.90) per 100 person-years) (HR 1.02; 95% CI 0.89-1.17; P <0.001 for noninferiority).
There was no significant difference in the risk for all-cause mortality or non-CV death with linagliptin vs. placebo.
Rates of hospitalization for heart failure did not differ between treatment groups: 6.0% and 6.5% in the linagliptin and placebo groups, respectively (HR 0.90; 95% CI 0.74-1.08; P=0.26).
The secondary renal outcome occurred in 9.4% and 8.8% of patients in the linagliptin and placebo groups, respectively (absolute incidence rate difference, 0.22 (95% CI −0.52 to 0.97) per 100 person-years) (HR 1.04; 95% CI, 0.89-1.22; P=0.62).
Linagliptin did not affect the risk for sustained ≥40% reduction in eGFR, sustained ESKD, or death due to kidney disease, but significantly reduced the risk for progression to albuminuria (HR 0.86; 95% CI 0.78-0.95; P=0.0034).
There were 9 (0.3%) vs. 5 (0.1%) events of adjudication-confirmed acute pancreatitis in the linagliptin and placebo groups, respectively.
In patients with type 2 diabetes at high risk of CV events and a high prevalence of kidney disease, linagliptin added to usual care was noninferior to placebo added to usual care for the primary outcome of 3-point MACE and did not demonstrate evidence of CV benefit.
There was no significant benefit of linagliptin compared with placebo for the incidence of the secondary kidney composite outcome.
Linagliptin showed no increase in risk of hospitalization for heart failure, even in patients at high risk of heart failure.
Linagliptin demonstrated a reassuring long-term kidney safety profile, with a reduction in progression of albuminuria.
Key Messages/Clinical Perspectives
Linagliptin demonstrated a long-term CV safety profile in patients with type 2 diabetes, including those with CV and/or kidney disease.
Perkovic V, Jardine MJ, Neal B, et al. Linagliptin Effects on Heart Failure and Related Outcomes in Individuals With Type 2 Diabetes Mellitus at High Cardiovascular and Renal Risk in CARMELINA. Circulation. 2019 Jan 15;139(3):351-61.
Present disclosure: S.E. Kahn: Boehringer Ingelheim, Eli Lilly, Intarcia, Janssen, Merck, Novo Nordisk, Neurimmune. N. Marx: Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Merck Sharp & Dohme, Sanofi-Aventis, Boehringer Ingelheim, Eli Lilly, Novo Nordisk. D.K. McGuire: Eisai, Eli Lilly, Janssen, AstraZeneca, Boehringer Ingelheim, Lexicon, Merck Sharp & Dohme, Novo Nordisk, Sanofi-Aventis. R.D. Toto: Relypsa, Akebia, AstraZeneca, Bayer, Boehringer Ingelheim, Quest Diagnostic, Vifor, WebMD. C. Wanner: Bayer, Boehringer Ingelheim, Merck Sharp & Dohme, AstraZeneca, Eli Lilly, Mitsubishi Tanabe. M.E. Cooper: AstraZeneca, Eli Lilly, Boehringer Ingelheim, Servier, Novo Nordisk, Bayer, Merck Sharp & Dohme, Novartis.
Jose C. Florez, MD, PhD
Chair, ADA Scientific Sessions Meeting Planning Committee
The 79th American Diabetes Association’s Scientific Sessions were held in San Francisco, California from June 7-11, 2019. The meeting was attended by over 15,000 professional attendees from 115 countries, … [ Read all ]
Presented by: Kimberly L. Drews, MD, PhD; Lorraine E. Levy Katz, MD; Petter Bjornstad, MD; Neil H. White, MD; Jeanie B. Tryggestad, MD; Ruth S. Weinstock, MD, PhD; for the TODAY2 Study Group
Presented by: Gilles R. Dagenais, MD; Rafael Diaz, MD; Matthew C. Riddle, MD; Hertzel C. Gerstein, MD, MSc; Helen Colhoun, MD; Jeffrey L. Probstfield, MD; Hertzel C. Gerstein, MD, MSc
Presented by: Vanita R. Aroda, MD; Richard E. Pratley, MD; Stephen C. Bain, MA, MD, FRCP; Mansoor Husain, MD, FRCPC; John B. Buse, MD, PhD; Vivian Fonseca, MD
Presented by: Alison B. Evert, MD; Janice MacLeod, MA, RDN, CDE; William S. Yancy, Jr., MD, MHS; W. Timothy Garvey, MD; Ka Hei Karen Lau, MS, RD, LDN, CDE; Christopher D. Gardner, PhD; Kelly M. Rawlings, MS


 中文
中文 Español
Español Italiano
Italiano Australia
Australia Argentina
Argentina Brazil
Brazil Lebanon
Lebanon Switzerland
Switzerland